AUA: Upper Tract Urothelial Carcinoma (2023)
Jump to navigation
Jump to search
- Literature search up to January 2023
*****All of the information below is contained in the more comprehensive Upper Urinary Tract Urothelial Cancer Chapter Notes*****
Background[edit | edit source]
- UTUC refers to urothelial tumors that originate from the inner lining of the ureter, calyces, or renal pelvis
- Estimated annual incidence in US: 7,000
- Slightly less than annual incidence of testicular cancer: 8,000-10,000
- Peak incidence is seen in adults aged >70 years
- 3x more common in males than females in western countries
- Risk factors (5):
- Occupational exposure
- Geographic location
- Balkan endemic nephropathy associated with aristolochia herbal ingestion
- Chronic upper tract inflammation
- Hereditary factors such as Lynch and Lynch-like syndrome
- At the time of diagnosis
- ≈25% will present as localized disease
- >50% will present as regionally advanced cancers
- ≈20% will present as distant disease
Diagnosis and Evaluation[edit | edit source]
Urologyschool.com Summary[edit | edit source]
- History and Physical Exam (1):
- Personal and family history
- To identify known hereditary risk factors for familial diseases associated with Lynch Syndrome
- Personal and family history
- Laboratory (2):
- Selective ipsilateral upper tract urine cytology
- Estimated GFR/Serum Cr
- Imaging (1):
- CT urogram
- Metastatic staging [not discussed in guidelines]
- Other (3):
- Cystoscopy to assess lower urinary tract
- Upper tract endoscopy and biopsy
- Universal histologic testing of UTUC with additional studies, such as immunohistochemical or microsatellite instability
History and Physical exam[edit | edit source]
- History
- Personal and family history to identify known hereditary risk factors for familial diseases associated with Lynch Syndrome
- If positive, referral for genetic counseling should be offered.
- Patients with Lynch Syndrome undergo routine screening due to increased life-long risk for developing associated malignancies, often occurring before 50 years of age
- Lynch syndrome
- Familial, autosomal-dominant multi-organ cancer syndrome
- Due to an inherited germline mutation in a group of DNA damage response genes responsible mismatch repair (MMR), specifically MLH1, MSH2, MSH6, PMS2, or EPCAM
- Alterations affecting the normal function of these genes results in an accumulation of DNA errors and increases the potential for cancer development
- Accounts ≈7-20% of UTUC cases in the U.S
- Lynch syndrome may increase the possibility of contralateral upper tract involvement, which is an important potential clinical consideration when developing a treatment plan.
- Associated cancers (11):
- Colorectal (20-80%)
- Urothelial (1-18%)
- Gastric cancers (1-13%)
- Endometrial (15-60%) in females
- Ovarian cancer (1-38%) in females
- Biliary
- Small bowel
- Pancreatic
- Prostate
- Skin
- Sebaceous adenoma, sebaceous epithelioma, sebaceous adenocarcinoma, keratoacanthoma, and squamous cell carcinoma[1]
- Brain
- If positive, referral for genetic counseling should be offered.
- Personal and family history to identify known hereditary risk factors for familial diseases associated with Lynch Syndrome
Laboratory[edit | edit source]
- Selective ipsilateral upper tract urine cytology
- Provides supplemental histologic data to tumor biopsies
- High-grade cytology in the setting of low-grade biopsy findings indicates the likely presence of higher-risk features (e.g., high-grade tumor) missed on biopsy sampling.
- Specimen collection considerations
- Can be obtained either as barbotage (saline irrigation and aspiration) or by saline irrigation with passive collection (washings)
- Preferred over a voided urinary specimen, due to (3)
- Improve cellular yield
- Avoid potential contamination in case of concomitant bladder and/or prostatic urethral disease
- Avoid theoretical dilution of the specimen from a normal contralateral unit
- Preferred over a voided urinary specimen, due to (3)
- Should be collected prior to any contrast use to avoid artifactual cellular changes from contrast solutions
- Collecting selective cytology after tumor biopsy can improve the yield of cells for cytologic analysis.
- Can be obtained either as barbotage (saline irrigation and aspiration) or by saline irrigation with passive collection (washings)
- Urine cytology is reported according to 7 categories (Paris System):
- Non-diagnostic
- Negative for high-grade urothelial carcinoma
- Atypical urothelial cells
- Suspicious for high-grade urothelial carcinoma
- High-grade urothelial carcinoma
- Low-grade urothelial neoplasm
- Other malignancies
- Provides supplemental histologic data to tumor biopsies
- Assessment of renal function
- Can help with patient counseling, strategizing treatment sequence (operative approach and administration of systemic therapy), and determination of downstream risks of CKD and potential dialysis.
- Recommended test: serum creatinine (to calculate an eGFR)
- For more refined evaluation, split function testing such as with differential renal scan or CT volumetric studies may be considered.
- The two formulas for monitoring eGFR commonly reported in the contemporary literature at this time are the Modification of Diet in Renal Disease and CKD – Epidemiology Collaboration (CKD-EPI) equations.
- UTUC with associated hydronephrosis
- Implications on assessment of renal function
- Caused by tumor obstruction may falsely under-estimate preoperative renal function and alter decision-making around the use of neoadjuvant chemotherapy (NAC).
- Atrophy of the contralateral (unaffected) renal unit may lead to over-estimates of postoperative renal function in the setting of NU since the kidney with lower differential function will remain in situ
- Renal decompression either by indwelling ureteric stent or a percutaneous nephrostomy tube placed in an uninvolved renal calyx along with oral fluid hydration for 7-14 days before re-checking eGFR will help to establish a more accurate estimation of baseline renal function.
- Ureteric stenting is the preferred method of drainage
- Percutaneous nephrostomy tubes in the setting of UTUC increases risk of tract seeding and has worse quality of life
- Ureteric stenting is the preferred method of drainage
- Implications on assessment of renal function
Imaging[edit | edit source]
- Cross-sectional imaging of the upper tract with contrast including delayed images
- Preferred modality: multiphase computed tomography (CT) scan with excretory phase imaging of the urothelium
- Pooled sensitivity of 92%
- Pooled specificity of 95%
- If contraindications to contrast-enhanced CT such as chronic kidney disease (CKD) (e.g. eGFR <30[2]) or untreatable allergy to iodinated contrast medium, use magnetic resonance (MR) urography
- MRI is less sensitive than CT, similar specificity
- If contraindications to multiphasic CT and MR urography, use retrograde pyelography in conjunction with non-contrast axial imaging (renal ultrasound) to assess the upper urinary tracts.
- Preferred modality: multiphase computed tomography (CT) scan with excretory phase imaging of the urothelium
- PET scans
- Should not be obtained routinely
- May be selectively considered for patients who are at risk for metastatic recurrence and are not able to have contrast enhanced CT and MRI
- Patients with findings suggestive of metastatic UTUC should be evaluated to define the extent of disease and referred to medical oncology for further management
Other[edit | edit source]
- Cystoscopy to assess lower urinary tract
- Essential component of the evaluation for patients with suspected UTUC due to the risk of concurrent lower tract urothelial cancer in this population
- Upper tract endoscopy +/- biopsy of any identified lesion
- Diagnostic ureteroscopy
- Indications for ureteroscopy or percutaneous endoscopy of the upper urinary tract (and when diagnostic and prognostic details are needed)
- Lateralizing hematuria
- Suspicious selective cytology
- Radiographic presence of a mass or urothelial thickening
- Document key descriptive features of UTUC that may guide further diagnostic testing and inform therapeutic interventions as well as provide points of comparison for subsequent ureteroscopic surveillance including:
- Location (ureteral segment, renal pelvis, calyceal sites and lower tract)
- Size
- Number
- Focality
- Appearance (sessile, papillary, flat/villous)
- Quality of visualization
- Can impact the accuracy of endoscopic inspection (e.g., bleeding, difficulty in access, tumor location, artifacts from instrumentation) and should be documented in endoscopic reports.
- See checklist in Guidelines Statement 2,Table 3: Standardized Upper Tract Endoscopy Suggested Reporting Elements
- Indications for ureteroscopy or percutaneous endoscopy of the upper urinary tract (and when diagnostic and prognostic details are needed)
- Biopsy of any identified lesion
- Approaches (2):
- Ureteroscopic biopsy with forceps
- Fluoroscopically guided retrograde brush biopsy
- Mucosal abnormalities may be difficult to biopsy effectively
- Attempted tissue confirmation may be facilitated with the use of brush biopsies or percutaneous image-guided biopsy.
- Approaches (2):
- Rare situations where endoscopic upper tract evaluation may not be necessary (2)
- Findings would not influence decision-making, such as patients with severe co-morbidities who are ineligible for intervention or request expectant management.
- Other diagnostic means clearly confirm the diagnosis of UTUC and thus histologic tissue confirmation is not clinically required.
- Example would include high-grade (HG) selective cytology or other source of tissue diagnosis, and clear and convincing radiographic findings of upper tract urothelial-based tumor(s) such as an obvious enhancing, urothelial based soft-tissue filling defect on contrast-enhanced imaging with urography.
- Such situations may be particularly relevant in patients with a history of HG urothelial cancer.
- Example would include high-grade (HG) selective cytology or other source of tissue diagnosis, and clear and convincing radiographic findings of upper tract urothelial-based tumor(s) such as an obvious enhancing, urothelial based soft-tissue filling defect on contrast-enhanced imaging with urography.
- If concomitant lower tract tumors (bladder/urethra) are discovered at the time of ureteroscopy, the lower tract tumors should be managed in the same setting as ureteroscopy.
- Consensus on prioritization of procedure sequencing (managing bladder before or after same-setting ureteroscopy) is lacking and heavily scenario-dependent.
- Rationale for managing the bladder first:
- Optimizing visualization within the bladder
- Avoiding back-pressure or back-washing into the upper tract in the case of post-ureteroscopy stenting
- Permitting final confirmation of bladder hemostasis.
- Addressing the upper tract first may be preferred in cases of
- Bulky bladder tumor involvement where complete resection is not possible
- Bulky upper tract disease in which risk assessment is the priority.
- Rationale for managing the bladder first:
- Some advocate use of ureteral access sheaths to reduce risk of seeding of tumors from bladder to upper tract or from upper tract to the lower tract
- The benefits of this approach require further prospective study.
- Consensus on prioritization of procedure sequencing (managing bladder before or after same-setting ureteroscopy) is lacking and heavily scenario-dependent.
- In cases of existing ureteral strictures or difficult access to the upper tract, minimize risk of ureteral injury by using gentle dilation techniques such as temporary stenting (pre-stenting) and limit use of aggressive dilation access techniques such as ureteral access sheaths.
- Perforation or disruption of the urothelium in patients with UTUC can risk tumor seeding outside the urinary tract.
- Recognized perforation or injury events should be documented with immediate cessation of the procedure as soon as safely possible with additional steps to limit sequelae (e.g., stenting, bladder decompression with urethral catheter drainage to limit reflux, nephrostomy tube placement in cases of a completely obstructive ureteral tumor and evidence of contrast extravasation).
- Precautionary measures in cases of difficult ureteral access such as avoiding dilation or placing a stent without performing ureteroscopy and then returning one-two weeks later to repeat the procedure (pre-stenting) can decrease the risk of iatrogenic injury and provide opportunity for a safer and more successful procedure.
- Perforation or disruption of the urothelium in patients with UTUC can risk tumor seeding outside the urinary tract.
- In cases where ureteroscopy cannot be safely performed or is not possible, an attempt at selective upper tract washing or barbotage for cytology may be made and pyeloureterography performed in cases where good quality imaging such as CT or MR urography cannot be obtained.
- When endoscopic examination of the involved upper tract is not possible, findings from selective cytology and retrograde pyelography may provide useful, objective and sufficient information for risk stratification .
- Example scenarios may include washings taken at the time of percutaneous nephrostomy tube placement or during attempted retrograde ureteroscopy that is abandoned for safety concerns.
- When endoscopic examination of the involved upper tract is not possible, findings from selective cytology and retrograde pyelography may provide useful, objective and sufficient information for risk stratification .
- At the time of ureteroscopy for suspected UTUC, ureteroscopic inspection of a radiographically and clinically normal contralateral upper tract should not be performed.
- Endoscopic procedures have risks for patient injury and the potential for tumor seeding in the presence of urothelial cancer. Performing upper tract endoscopy in the setting of a completely normal contralateral upper urinary tract without clinical indication or as a “screening” procedure is unnecessary, placing patients at undue risk and should not be performed
- Diagnostic ureteroscopy
- Universal histologic testing of UTUC with additional studies, such as immunohistochemical (IHC) or microsatellite instability (MSI)
- Routine tissue testing provides a more sensitive, first-line means to identify Lynch syndrome-associated features in tumor samples
- Immunohistochemical testing
- Can preliminarily identify the altered proteins associated with Lynch syndrome, and thus help to identify patients who may have the syndrome, who then require confirmation with further genetic (germline) testing
- Widely available
- Microsatellite instability
- Identifying the presence of Lynch syndrome-associated and MSI-high cancers also has clinical implications related to therapeutic treatment options, including identified sensitivity of urothelial cancers with mutations in DNA damage repair genes to systemic agents such as immune checkpoint inhibitors and cisplatinum-based chemotherapy
- Immunohistochemical testing
- Routine tissue testing provides a more sensitive, first-line means to identify Lynch syndrome-associated features in tumor samples
Optional[edit | edit source]
- Urine fluorescence in situ hybridization (FISH)
- May be considered adjunctively to adjudicate atypical or suspicious cytology results.
- Retrograde pyelograms
- Provide a roadmap for evaluation and possibly planning kidney-preserving strategies
- Should be considered at initial evaluation with images retained in the patient record
Risk Stratification[edit | edit source]
- Categorized as high- vs. low-risk of disease progression and pathologic stage ≥T2 disease
- Based on biopsy grade
- Association of high grade tumor on ureteroscopic biopsy with high-stage disease (≥pT2) on final pathology
- Positive predictive value: 60%
- Negative predictive value:77%
- Association of high grade tumor on ureteroscopic biopsy with high-stage disease (≥pT2) on final pathology
- Sub-stratified into favorable vs. unfavorable (see Table 4), based on (4):
- Cytology
- Radiographic appearance
- Multifocality
- Size
- Invasive features
- Heterogenous texture on enhanced and even unenhanced CT imaging has been associated with invasive disease
- Obstruction of the urinary tract
- Locoregional progression such as suspicious lymphadenopathy
- Presence of metastatic disease
- Endoscopic appearance
- Multifocality
- Size
- Tumors ≥ 1.5 cm in size are associated with a > 80% risk of invasive disease
- Measurement in the pre-surgical setting is not standardized and has not been shown to be independent of other more easily determined clinically identified features such as multifocality, invasion and obstruction.
- Appearance (sessile, papillary, flat/villous)
- Lower tract involvement
- Pan-urothelial disease as indicated by history of prior cystectomy, concomitant or metachronous lower tract urothelial cancer or contralateral UTUC diagnosis
- Based on biopsy grade
Management[edit | edit source]
UrologySchool.com Summary[edit | edit source]
- If low-risk
- Favorable
- Tumor ablation (preferred)
- Unfavorable
- Tumor ablation (optional)
- Surgical removal (radical nephroureterectomy or segmental ureterectomy)
- If low-risk and complete endoscopic ablation not feasible, chemoablation (in-situ tissue destruction) with mitomycin containing reverse thermal gel can be a treatment alternative
- Favorable
- If high-risk
- Favorable
- Surgical removal
- Tumor ablation (optional)
- Select patients who have low-volume tumors or cannot undergo RNU
- Unfavorable
- Surgical removal
- For surgically eligible patients with HR and unfavorable LR cancers endoscopically confirmed as confined to the lower ureter in a functional renal unit, distal ureterectomy with ureteral reimplant is the preferred treatment
- Favorable
Patient counseling[edit | edit source]
- Discuss and facilitate smoking cessation, if applicable, with patients at the time of diagnosis and treatment.
- Risk factors such as smoking are associated with advanced disease stage, recurrence and worse cancer-specific mortality among patients with UTUC, with the highest risk among current smokers.
- Provide patients with a description of the short- and long-term risks associated with recommended diagnostic and therapeutic options, including
- Need for endoscopic follow-up
- Urothelial recurrences are common in the management of UTUC, regardless of approach, and mandate long-term surveillance for which patients must be prepared – including the potential need for additional treatments.
- Risks of treatment
- Risk of clinically significant strictures with endoscopic management
- Ablative options can provide local control including durable long-term kidney sparing outcomes but incur additional endoscopic surveillance requirements and associated risks such as stricture and infection
- Use of chemoablative treatment with the reverse thermo-hydrogel preparation of mitomycin for pyelocaliceal instillation for LG tumors carries an FDA label warning for ureteral obstruction (>44%), bone marrow suppression, and embryo-fetal toxicity.
- Risk of post-nephroureterectomy CKD or dialysis
- Risk factors for post-operative development of CKD or progression of pre-existing CKD (8):
- Older age
- Diabetes mellitus
- Hypertension
- Male sex
- Obesity
- Tobacco use
- Larger tumor size
- Post-operative acute kidney injury.
- Perioperative nephrology consultation can be considered, particularly in patients with pre-existing kidney disease.
- Indications for referral to nephrology (4):
- eGFR < 45 mL/min/1.73m2
- Confirmed proteinuria
- Diabetics with preexisting CKD
- If eGFR is expected to be < 30 mL/min/1.73m2 after intervention.
- Indications for referral to nephrology (4):
- In patients with pre-existing CKD or a solitary kidney, attempts to preserve renal function can be made, if oncologically feasible and appropriate, with segmental or endoscopic organ-sparing approaches which preferentially are associated with improved postoperative renal function.
- In patients with sufficiently poor CKD in which NU could precipitate ESRD, a post operative plan for dialysis in conjunction with nephrology colleagues should be in place preoperatively including plans for dialysis access. Referral to nephrology for detailed evaluation and recommendations for perioperative management is warranted in such cases
- Risk factors for post-operative development of CKD or progression of pre-existing CKD (8):
- Side effects from neoadjuvant and adjuvant therapies.
- Risk of clinically significant strictures with endoscopic management
- Need for endoscopic follow-up
Kidney Sparing Management/Tumor Ablation[edit | edit source]
Indications[edit | edit source]
- Preferred
- Initial management for LR favorable UTUC, when technically feasible
- Observational studies suggest similar cancer-specific survival, similar complication rates, and improved renal function outcomes with endoscopic ablation, compared to nephroureterectomy
- Initial management for LR favorable UTUC, when technically feasible
- Optional
- Initial management for LR unfavorable UTUC and select patients with HR favorable disease who have low-volume tumors or cannot undergo RNU
- If low-risk and complete endoscopic ablation not feasible, chemoablation (in-situ tissue destruction) with mitomycin containing reverse thermal gel can be a treatment alternative
- High risk of ureteric stenosis with instillation of mitomycin containing reverse thermal gel
Technical considerations[edit | edit source]
- Approach
- May be accomplished via a retrograde or antegrade percutaneous approach
- Antegrade approach typically reserved for
- Larger tumors
- Tumor difficult to access in a retrograde fashion
- Patients who have undergone prior radical cystectomy or urinary diversion
- Antegrade approach typically reserved for
- May be accomplished via a retrograde or antegrade percutaneous approach
- Tumor size
- Tumors < 1.5 cm in size may be optimal for endoscopic ablation given a lower risk of invasive disease.
- Tumors ≥ 1.5 cm in size are associated with a > 80% risk of invasive disease
- Larger tumors (≥ 1.5 cm) may be considered for ablation based on the provider’s experience and assessment of the need for kidney sparing surgery.
- Tumors < 1.5 cm in size may be optimal for endoscopic ablation given a lower risk of invasive disease.
- Energy source
- Thulium laser, holmium laser, Neodymium (Nd:YAG), and electrocautery devices (e.g., Bugbee) may all be deployed through an endoscope.
- Chemoablation
- May be employed either through retrograde ureteral catheter instillation or percutaneous access with fluoroscopic imaging guidance
- Ureteral access sheath
- Prior to placement of any ureteral access sheath, the entire ureter should be directly visualized in order to avoid missing any luminal neoplasms, especially in the distal ureter
- Advantages (3):
- Allows for repeated scope passage up and down the ureter for sampling
- Means of fluid egress from the upper tract to avoid excess pelvicalyceal hydrostatic pressure from irrigation solutions
- Lower rate of intravesical recurrence (based on observational study)
Adjuvant therapy[edit | edit source]
Pelvicalyceal or intravesical chemotherapy following ablation of UTUC tumors[edit | edit source]
- Considered optional
- Principle of an immediate instillation of intravesical or pyelocaliceal (upper tract) chemotherapy at the time of endoscopic tumor ablation for UTUC is undertaken by extrapolation of the data supporting immediate instillation of intravesical chemotherapy at the time of transurethral resection of a bladder tumor
- Prior to administration, must confirm that there is no perforation of the bladder or upper tract
- Approaches
- Antegrade perfusion by nephrostomy tube
- Retrograde perfusion via ureteral catheter
- Bladder instillation by transurethral catheter with reflux via a double J ureteral stent.
- In the third scenario, a cystogram and demonstration of adequate reflux of contrast into the pyelocaliceal system is recommended.
Pelvicalyceal BCG[edit | edit source]
- May be offered to patients with HR favorable UTUC after complete tumor ablation or patients with upper tract carcinoma in situ (CIS).
- Consists of a 6-week induction course of BCG
- Imperative indications
- Solitary kidney status
- Bilateral UTUC
- RIsk of progression to end-stage renal disease
Repeat endoscopic evaluation[edit | edit source]
- Should be performed within 3 months
- Proclivity of UTUC to recur and for residual disease to remain after the first ablation
- A 30-day window on either side of this endpoint (i.e., 30 to 90 days) is justified to allow timely identification of recurrences and may be dictated by aspects such as tumor size, visualization, access, treatment efficacy, etc., as clinically indicated
- If residual disease identified, repeat endoscopic assessment should occur within 3-month intervals until no evidence of upper tract disease is identified.
- In patients with LR UTUC with evidence of risk group progression (tumor size, focality, or grade) or when tumor ablation is not feasible, further endoscopic-assisted attempts are not recommended. surgical resection of all involved sites either by RNU or segmental resection of the ureter should be offered.
Surgical Removal[edit | edit source]
Indications[edit | edit source]
- Preferred
- Surgically eligible patients with HR UTUC
Approaches[edit | edit source]
- Radical nephroureterectomy with complete bladder cuff excision (BCE)
- RNU with complete bladder cuff excision and lymphadenectomy is the standard of care for patients with HR UTUC.
- Segmental ureterectomy
Radical nephroureterectomy[edit | edit source]
- Principles
- Complete excision of ipsilateral upper tract urothelium, including the intramural portion of the ureter and ureteral orifice with negative margins
- Specimen should be removed en bloc whenever technically feasible
- Avoidance of urinary spillage, such as by early low ligation of the ureter, to minimize the risk of seeding urothelial cancer outside the urinary tract.
- Complete excision of ipsilateral upper tract urothelium, including the intramural portion of the ureter and ureteral orifice with negative margins
- Approach
- Open, robotic, and laparoscopic approaches are suitable
- Minimally invasive approaches were associated with favorable perioperative outcomes including shorter length of stay and fewer complications, and, therefore, are favored for most patients when principles of RNU can be maintained
- Consider open surgical approaches for large, bulky UTUC with clinical evidence for direct invasion to adjacent structures
- Open, robotic, and laparoscopic approaches are suitable
- Bladder cuff excision
- Worse local and metastatic recurrence rates with associated decreased CSS and OS for patients who did not receive complete BCE.
- Approach
- Extravesical or transvesical l (e.g., midline cystotomy)
- Open, minimally invasive or transurethral endoscopic techniques.
- Transurethral endoscopic approaches are associated with higher recurrence rates in the bladder and may limit the ability to utilize post-NU intravesical therapies if the bladder is not fully closed
- Complication rates following RNU
- Range from 15% to 50%
- 30-day mortality risk of 1%
Ureterectomy[edit | edit source]
- Options
- Segmental ureterectomy with ureteroureterostomy
- Small, unifocal tumors (typically 1 cm or smaller) tumors isolated to a short segment of the proximal or mid-ureter requiring resection of ≤2 cm or less of ureteral length to allow for primary ureteroureterostomy.
- Longer sections of ureteral involvement and resection may require more complex reconstruction techniques when kidney sparing is desired.
- Small, unifocal tumors (typically 1 cm or smaller) tumors isolated to a short segment of the proximal or mid-ureter requiring resection of ≤2 cm or less of ureteral length to allow for primary ureteroureterostomy.
- Distal ureterectomy with ureteral reimplant
- Preferred treatment for surgically eligible patients with HR and unfavorable LR cancers endoscopically confirmed as confined to the lower ureter in a functional renal unit
- Tumor ablation considered alternative options to the gold-standard of extirpative resection
- Tumor ablation may yield less optimal results and require multiple additional procedures
- Tumor ablation considered alternative options to the gold-standard of extirpative resection
- Most favorable candidates for distal ureterectomy are patients who
- Have ureteral tumors in the lower third of the ureter
- Sufficiently mobile bladder with capacity to facilitate reimplantation with or without reconfiguration of the bladder to facilitate a tension-free anastomosis (i.e., Boari flap or psoas hitch maneuver).
- Preferred treatment for surgically eligible patients with HR and unfavorable LR cancers endoscopically confirmed as confined to the lower ureter in a functional renal unit
- Segmental ureterectomy with ureteroureterostomy
- Reasonable alternatives to RNU for well-selected patients
- Principles
- Patient counseling to describe techniques, potential requirements for urinary reconstruction and associated complications including the potential impact on postoperative bladder function.
- Preoperative endoscopic assessment to evaluate sites of involvement and proximal extent of disease.
- Preoperative assessment of bladder capacity and function in cases where more extensive reconstruction such as a Boari flap are anticipated to permit a tension free ureterovesical anastomosis or the use of bowel segments.
- Intraoperative pathologic assessment (i.e., frozen sections) of proximal and distal margins to ensure complete resection with negative margins.
- Reasonable attempts to avoid of spillage of urine into the surgical field.
- Watertight, tension free closure to facilitate functional healing and avoid urine leak (of urine potentially contaminated with malignant cells).
- When performing NU or distal ureterectomy, the entire distal ureter including the intramural ureteral tunnel and ureteral orifice should be excised, and the urinary tract should be closed in a watertight fashion.
- The resultant hiatus in the bladder in the location of the excised ureteral orifice with or without the bladder cuff can be closed formally in a watertight fashion in one or more layers
- A formal BCE with watertight closure of the bladder cuff should be performed to
- Avoid urinary extravasation from the bladder
- Facilitate more rapid catheter removal
- Permit instillation of intravesical adjuvant chemotherapy in the perioperative setting
- Delayed closure by secondary intension in a decompressed bladder without formal bladder closure has also been described.
- A formal BCE with watertight closure of the bladder cuff should be performed to
- The resultant hiatus in the bladder in the location of the excised ureteral orifice with or without the bladder cuff can be closed formally in a watertight fashion in one or more layers
Lymph node dissection[edit | edit source]
- If HR UTUC, LND recommended
- No RCTs to evaluate the effect of LND on oncologic outcomes in patients undergoing NU or SU
- Sufficient non-randomized evidence to suggest an oncologic benefit to LND at the time of NU for patients with “HR” stratification by guidelines
- Recommended minimal templates in non-metastatic disease
- Tumors in the pyelocaliceal system: lymph nodes of the ipsilateral great vessel extending from the renal hilum to at least the inferior mesenteric artery.
- Tumors in the proximal 2/3 of the ureter: lymph nodes of the ipsilateral great vessel extending from the renal hilum to the aortic bifurcation.
- Tumors in the distal 1/3 of the ureter: ipsilateral pelvic LND to include at minimum the obturator and external iliac nodal packets.
- Internal and common iliac nodal packets may be removed in the appropriate clinical setting.
- Limited data suggest cranial migration of lymph node metastases to the ipsilateral great vessels such that higher dissection may be considered in the appropriate clinical setting and per clinician judgement
- If LR UTUC, LND optional
- Limited evidence exists to support a beneficial role for LND at time of NU or ureterectomy among patients with LR UTUC
Neoadjuvant/Adjuvant Chemotherapy and Immunotherapy[edit | edit source]
Adjuvant intravesical chemotherapy[edit | edit source]
- In patients undergoing RNU or SU (including distal ureterectomy) for UTUC, a single dose of perioperative intravesical chemotherapy should be administered in eligible patients to reduce the risk of bladder recurrence.
- The exact timing of therapy has varied including instilling intravesical chemotherapy at the time of catheter removal (ODMIT-C trial), while other retrospective series reported instillation during surgery or up to 48 hours postoperatively.
- Little data to support one intravesical chemotherapeutic over another.
- Many use gemcitabine over mitomycin due to risks of chemical peritonitis with extravesical extravasation of MMC
Systemic chemotherapy[edit | edit source]
Neoadjuvant systemic chemotherapy[edit | edit source]
- Cisplatin-based neoadjuvant chemotherapy should be offered to patients undergoing RNU or ureterectomy with HR UTUC, particularly in those patients whose post-operative eGFR is expected to be <60 mL/min/1.73m2 or those with other medical comorbidities that would preclude platinum-based chemotherapy in the post-operative setting.
- The strongly positive data from these phase II trials, the established high-level evidence seen in bladder cancer trials, the consistent findings from pooled meta-analytic data, and the compelling clinical challenges imposed by post-RNU renal function on cis-platinum eligibility support the standard use of NAC regimens for HR UTUC.
- In the neoadjuvant setting, dosing regimens may be better tolerated, allowing more courses to be completed, and permitting patients to proceed to appropriate surgical intervention.
- Alternatives to cisplatin-based chemotherapy (i.e., immune checkpoint inhibitors, carboplatin, antibody drug conjugates, targeted FGFR therapies) are not recommended in the neoadjuvant setting (prior RNU or ureterectomy) outside of clinical trials
Adjuvant systemic chemotherapy[edit | edit source]
- Platinum-based adjuvant chemotherapy should be offered to patients with advanced pathological stage (pT2–T4 pN0–N3 M0 or pTany N1–3 M0) UTUC after RNU or ureterectomy who have not received neoadjuvant platinum-based therapy
- Adjuvant platinum-based chemotherapy for select patients with UTUC post-RNU is a standard based on results from the randomized phase III POUT trial.
- Subjects in the adjuvant chemotherapy arm had improved DFS and lower risk of metastases or death, compared with those on observation.
- A subgroup analysis demonstrated that outcomes for patients with lymph node involvement and those treated with carboplatin chemotherapy were worse than those without positive nodes or treated with cisplatin chemotherapy
- Carboplatin remains a reasonable choice for HR cisplatin-ineligible patients post-RNU if NAC was not given
- Adjuvant platinum-based chemotherapy for select patients with UTUC post-RNU is a standard based on results from the randomized phase III POUT trial.
Adjuvant immunotherapy[edit | edit source]
- Adjuvant nivolumab therapy may be offered to patients who received neoadjuvant platinum-based chemotherapy (ypT2–T4 or ypN+) or who are ineligible for or refuse perioperative cisplatin (pT3, pT4a, or pN+)
- CheckMate 274 evaluated adjuvant nivolumab following surgery in patients with HR non-metastatic urothelial carcinoma
- Majority of patients underwent radical cystectomy for bladder primaries, 20% of patients underwent surgery for UTUC
- Inclusion criteria for both studies were patients with HR urothelial cancer defined as pT3, pT4a, or pN+ for patients who had not received neoadjuvant cisplatin-based chemotherapy and ypT2 to ypT4a or ypN+ for patients who had received neoadjuvant cisplatin
- Adjuvant nivolumab approved for UTUC and urothelial carcinoma of the bladder in patients with advanced disease identified from post-surgical pathology findings
- Adjuvant platinum-chemotherapy over adjuvant nivolumab is recommended for eligible patients who did not receive NAC. Scenarios for use of adjuvant nivolumab include:
- Patients with contraindications to platinum-based chemotherapy (e.g., poor renal function, performance status, sensorineural hearing loss, neuropathy or congestive heart failure, allergy)
- Patients with HR pathology after NAC
- Patients who refuse standard forms of adjuvant chemotherapy after appropriate counseling.
- CheckMate 274 evaluated adjuvant nivolumab following surgery in patients with HR non-metastatic urothelial carcinoma
Special scenarios[edit | edit source]
Watchful waiting or surveillance[edit | edit source]
- May be offered to select patients with UTUC with
- Significant comorbidities/competing risks of mortality
- Significant risk of End-Stage Renal Disease (ESRD) with any intervention resulting in dialysis.
- Discussion of treatment related risks including perioperative mortality may lead to a shared decision to proceed with active surveillance (whereby periodic assessments such as imaging or limited endoscopic assessment are performed) or watchful waiting/expectant management, where interventions are limited to palliation or awaiting symptomatic progression – especially in those with very limited life expectancy.
- In such cases, patients and family should be counseled and prepared for disease-related events such as bleeding, obstruction, infection, and pain with options for palliation that may be limited.
CIS limited to the region within the ureteral orifice[edit | edit source]
- Topical therapies such as BCG along with refluxing ureteral stenting that has been used for in cases of CIS near the ureterovesical junction or transurethral resection of the transmural portion of the ureter for very distal tumors, as an extension of bladder resection procedures, when tumor is limited to the region inside the ureteral orifice and not beyond the bladder wall, thus anatomically managed as bladder cancer
Advanced disease[edit | edit source]
Clinical, regional node-positive (N+)[edit | edit source]
- Should initially be treated with systemic therapy.
- Consolidative RNU or ureterectomy with lymph-node dissection may be performed in those with a partial or complete response.
- Pooled data from comparative outcomes utilizing NAC in patients with clinically node positive (cN+) disease supports this approach.
Distant metastatic disease (M+)[edit | edit source]
- Systemic therapy and alternative approaches (i.e., radiotherapy with or without chemotherapy in selected cases) should be favored for inoperable or symptomatic patients with M+ UTUC
- RNU or ureterectomy should not be offered as initial therapy
- Oncologic outcomes in the metastatic setting are strongly determined by response to systemic therapy, and surgical treatment has no demonstrable therapeutic efficacy for cytoreduction or as a single modality in this setting.
Unresectable UTUC[edit | edit source]
- Localized disease may be deemed unresectable or ineligible for extirpative surgical management due to significant medical comorbidities or other factors including refusal to accept surgical treatment (e.g., solitary kidney).
- Should be offered a clinical trial or best supportive care including palliative management (radiation, systemic approach, endoscopic, or ablative) for refractory symptoms such as hematuria.
- Formulating alternative care options should be approached with multi-disciplinary input with a focus on realistic goals of care such as providing means of local control for functional preservation (e.g., renal function) and palliation (e.g., bleeding, infection)
- Multi-modal approaches include combination of endoscopic management to maintain upper and lower tract function (e.g., stents, nephrostomies, ablation for bleeding and local control) in addition to systemic treatment options if available. Rarely, radiation, angioembolization, or percutaneous ablation for palliation of bleeding can be offered
Surveillance and Survivorship[edit | edit source]
Oncologic Surveillance[edit | edit source]
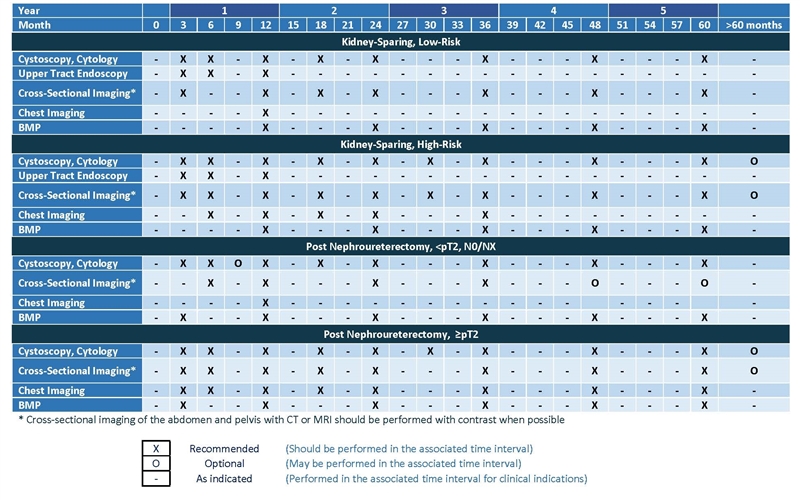
- See Table from Original Guidelines
- Consists of evaluation of potential recurrence in
- Lower urinary tract, through
- Cystoscopy
- Upper urinary tract, through
- Upper tract endoscopy
- Upper tract imaging
- Preferred modality: CT urogram
- If patient unable to receive iodinated contrast, use MR urography or retrograde pyelography combined with non-contrast axial imaging
- Preferred modality: CT urogram
- Urine cytology
- Chest (distant metastasis), though
- CXR or CT chest
- Lower urinary tract, through
{kind=link}
Surveillance after kidney sparing[edit | edit source]
- Low-risk patients managed with kidney sparing treatment
- Cystoscopy and upper tract endoscopy within 1-3 months of treatment to confirm successful treatment.
- If successful treatment confirmed (no evidence of disease), perform
- Cystoscopy of the bladder once again within the first year after treatment, then at least every 6-9 months for the first 2 years and then at least annually thereafter.
- Upper tract endoscopy at 6 months and 1 year [after treatment].
- Can be subsequently performed for any symptoms or significant findings on upper tract imaging.
- Upper tract imaging should be performed at least every 6-9 months for first 2 years, then annually up to 5 years.
- Surveillance after 5 years in the absence of recurrence should be based on shared decision-making.
- No distant metastatic evaluation since risk is low with low-risk disease
- High-risk patients managed with kidney sparing treatment
- Cystoscopy, upper tract endoscopy, and upper tract urine cytology within 1-3 months of treatment to confirm successful treatment.
- If successful treatment confirmed (no evidence of disease), perform
- Cystoscopy of the bladder and cytology at least every 3-6 months for the first 3 years and then every 6-12 months up to 5 years.
- Upper tract endoscopy should be performed at least at 6 months and 1 year [after treatment]
- Upper tract imaging and BMP should be performed every 3-6 months for 3 years, then every 6-12 months for 2 years, and then annually thereafter.
- Distant metastatic evaluation: Chest imaging (chest X-ray or CT) is recommended every 6-12 months to evaluate for intrathoracic metastasis up to 5 years following last diagnosis/treatment
- Surveillance after 5 years in the absence of recurrence should be based on shared decision-making.
- If patient develops urothelial recurrence in the bladder or urethra or positive cytology following kidney sparing treatment for UTUC, evaluate for possible ipsilateral recurrence or development of new contralateral upper tract disease.
Surveillance after radical nephroureterectomy[edit | edit source]
- Intravesical recurrence
- Rates of intravesical recurrence after nephroureterectomy: ≈29%
- Most recurrences occur within the first 2 years
- Unclear how long bladder surveillance should continue for after 2 years
- Most recurrences occur within the first 2 years
- Risk factors for intravesical recurrence:
- Male sex
- Previous bladder cancer
- Preoperative CKD
- Positive preoperative urinary cytology
- Ureteral tumor size
- Multifocality
- Invasive pathologic T-stage
- Presence of necrosis
- Laparoscopic approach
- Extravesical bladder cuff removal
- Positive surgical margins
- Prior ureteroscopic biopsy
- Given the substantial risk of local (bladder) recurrences within the first years following nephroureterectomy, risk adapted surveillance with cystoscopy and urine cytology at routine intervals is indicated to facilitate prompt detection of bladder recurrences.
- Rates of intravesical recurrence after nephroureterectomy: ≈29%
- Contralateral recurrence
- Risk of recurrence to the contralateral upper tract: ≈2%
- Locoregional, retroperitoneal, and distant metastases
- Risk factors
- Multifocality
- Stage T3-4
- Grade G3
- Presence of lymph node metastasis
- Intrabdominal recurrences
- Very low rates in low-risk patients
- In patients with HG disease, LVI, or tumor multifocality, periodic imaging of the abdomen and pelvis is warranted, particularly for the first 2 years
- Distant metastases
- Lung metastasis
- Low risk in patients with <pT2 N0/M0
- Can occur in patients with high-grade disease, so periodic chest imaging is warranted
- Chest imaging can be done via chest x-ray or CT
- Chest x-ray is likely sufficient, less costly, and associated with less radiation exposure
- Chest imaging can be done via chest x-ray or CT
- Bone
- Liver
- Brain
- Rare following nephroureterectomy
- Patients undergoing follow-up for HR UTUC following nephroureterectomy with acute neurological signs or symptoms should undergo prompt neurologic evaluation with cross-sectional imaging of the brain and/or spine by CT or MRI
- Lung metastasis
- Risk factors
- <pT2 N0/M0 managed with NU
- Cystoscopy and urine cytology within 3 months after surgery, then repeated based on pathologic grade.
- For LG this should repeated at least every 5-9 months for the first 2 years and then at least annually thereafter.
- For HG, this should be repeated at least every 3-6 months for the first 3 years and then at least annually thereafter.
- Cross-sectional imaging of the abdomen and pelvis should be done within 6 months after surgery and then at least annually for a minimum of 5 years
- Due to the metastasis risk and estimated 5% probability for contralateral disease
- Follow up after nephroureterectomy for patients with non-muscle invasive, node-negative UTUC should be largely focused on the risk of intravesical recurrence
- Surveillance after five years in the absence of recurrence should be encouraged and based on shared decision-making between the patient and clinician
- Cystoscopy and urine cytology within 3 months after surgery, then repeated based on pathologic grade.
- T2+ managed with NU
- Cystoscopy with cytology at 3 months after surgery, then every 3-6 months for 3 years, and then annually thereafter.
- Cross-sectional imaging of the abdomen and pelvis with multiphasic contrast-enhanced CT urography should be performed every 3-6 months for years 1 and 2, every 6 months at year 3, and annually thereafter to year 5.
- Chest imaging, preferably with chest CT, every 6-12 months for the first 5 years.
- Beyond five years after surgery in patients without recurrence, ongoing surveillance with cystoscopy and upper tract imaging may be continued on an annual basis according to principles of shared/informed decision-making
- Sequelae of nephroureterectomy
- Repeat assessment of blood pressure, eGFR, and proteinuria should be performed soon after nephroureterectomy then again in 3-6 months to assess for development or progression of CKD.
- With significant nephron mass loss, hyperfiltration can occur resulting in glomerular damage, exacerbation of proteinuria and progressive sclerosis with further decline in GFR.
- The long-term impact of renal dysfunction increases risks of osteoporosis, anemia, metabolic and cardiovascular disease, hospitalization and death.
- Effective treatment strategies are available to slow the progression of CKD and reduce cardiovascular risks, and therefore timely identification of progressive renal dysfunction and/or proteinuria can provide opportunity for medical intervention when indicated.
- Careful management of DM and HTN and avoidance of substantial weight gain may slow or prevent CKD progression and should be prioritized on a long-term basis
- Identifying modifiable risk factors including diabetes mellitus (DM), hypertension (HTN) and smoking is essential. Optimizing glycemic and blood pressure control, smoking cessation and minimizing risk of acute kidney injury (with avoidance of hypotension and nephrotoxic agents such as intravenous contrast or non-steroidal anti-inflammatory drugs) should reduce the degree of renal dysfunction in the perioperative period.
- In patients who develop progressive renal insufficiency or proteinuria should be referred to nephrology.
- Other laboratory evaluations (e.g., CBC, LDH, liver function tests, and alkaline phosphatase) may be obtained at the discretion of the clinician or if advanced disease is suspected.
- Repeat assessment of blood pressure, eGFR, and proteinuria should be performed soon after nephroureterectomy then again in 3-6 months to assess for development or progression of CKD.
Survivorship[edit | edit source]
- Discuss disease-related stresses and risk factors and encourage patients with urothelial cancer to adopt healthy lifestyle habits, including smoking cessation, exercise, and a healthy diet, to promote long-term health benefits and quality of life.
- UTUC is associated with metabolic syndrome and obesity, with obesity adversely impacting disease-specific outcomes among patients undergoing RNU.
- Clinicians should work with patients and their primary care providers to ensure that comorbidities are optimally managed throughout the course of care for UTUC and during surveillance to maximize quality of life during survivorship.
References[edit | edit source]
- Coleman, Jonathan A., et al. "Diagnosis and Management of Non-Metastatic Upper Tract Urothelial Carcinoma: AUA/SUO Guideline." The Journal of Urology 209.6 (2023): 1071-1081.